For most of our lives, we have pictured a heart attack the same way: an older man, clutching his chest, collapsing without warning. It was something that happened later in life, after decades of wear and tear. That picture is changing, and the change is worth understanding, especially if you have children, nieces, nephews, or grandchildren in their thirties and forties. Doctors across the country are now seeing heart attacks in people who, by any old-fashioned reckoning, should have been decades away from worrying about their hearts.
This is not a small shift. It is one of the more striking trends in modern medicine, and it touches families in a way that feels deeply unfair. A man of forty-two, fit-looking and busy with work and young kids, is simply not who we expect to see in a cardiac unit. Yet there he is, more and more often. Understanding why this is happening, what to watch for, and how these younger heart attacks are treated differently can make a real difference for the people you love.
The trend is real and it is measurable. Heart attacks in adults under fifty have been climbing steadily, even as heart attack rates in older adults have been falling. Among adults between the ages of eighteen and forty-four, heart attack rates have jumped by roughly two-thirds since 2019. A generation ago, only about one in ten heart attacks happened to someone under forty. Today that figure is closer to one in five, and the rate in this younger group has been creeping up by about two percent every single year.

Behind those numbers are some sobering shifts in everyday health. Obesity among young adults has risen from around a third of that age group to roughly forty percent in little more than a decade, with diabetes climbing in the same age band. Nearly half of all adults between twenty and forty-four now carry at least one major risk factor for heart disease. Perhaps most surprising of all, one in four young adults already has high blood pressure, often without knowing it. These are not problems that announce themselves. They build quietly, year after year, until one day they make themselves known in the worst possible way.
There is no single villain here. Instead, several forces have come together at the same time, and they reinforce one another. The two biggest drivers, the ones cardiologists point to first, are the twin epidemics of obesity and diabetes. Both have been spreading into younger and younger age groups. The trouble with developing these conditions early is not just the conditions themselves, but the sheer length of time the body is exposed to them. A person who has been heavy since their teens has, by age thirty-five, already put their blood vessels through twenty years of strain. That is two decades of high blood sugar, low-grade inflammation, and quiet damage to the lining of the arteries, all happening in a body that still looks young.

Lifestyle plays an enormous role. Long hours spent sitting, whether at a desk, behind the wheel, or in front of a screen, take a steady toll on the heart. Diets heavy in processed foods, fast food, sugary drinks, and unhealthy fats raise cholesterol and clog arteries faster than nature intended. Add in too little sleep, which fuels inflammation and disrupts the heart's rhythm, and you have a recipe for trouble brewing well before middle age.
Then there are the newer culprits, the ones that did not feature in the heart health conversations of decades past. Recreational drug use is a growing concern. A very large study released in 2025 found that cannabis users under fifty had a strikingly higher risk of heart attack, even when they had normal blood pressure, healthy cholesterol, and no history of smoking tobacco. Cocaine and methamphetamine carry their own serious cardiac dangers. Vaping, often assumed to be harmless, has been shown to stiffen and irritate blood vessels even when the liquid contains no nicotine at all.
Chronic stress and mental health deserve their own mention. The pressures of modern life, financial worry, work strain, anxiety, and depression all leave a mark on the heart. They raise the stress hormones that quietly damage blood vessels over time, and they often push people toward unhealthy habits as a way of coping. There is also growing evidence that infection with COVID-19 can leave lingering effects on the cardiovascular system, raising risk for months or even years afterward. And for some, the cards are dealt before birth. A strong family history of early heart disease, or an inherited cholesterol particle called lipoprotein(a), can raise the odds considerably regardless of how carefully a person lives.
One of the most dangerous things about heart attacks in younger people is that they are so easily dismissed. A thirty-eight-year-old with chest tightness is far more likely to blame heartburn, a pulled muscle, anxiety, or simple tiredness than to suspect his heart. That delay can be deadly, because the faster a heart attack is treated, the better the outcome.
The classic warning signs still apply, and everyone should know them. Chest discomfort or pressure, shortness of breath, and pain that spreads to the arm, jaw, neck, or back are all signals not to ignore. But the symptoms do not always arrive in that textbook form. Lightheadedness, unusual fatigue, a cold sweat, or nausea can all be part of the picture. This is especially true for women, who are more likely than men to experience these quieter, less obvious warning signs. The simple rule worth passing along to younger family members is this: if something feels seriously wrong and does not let up, it is always better to be checked and reassured than to wait and hope.
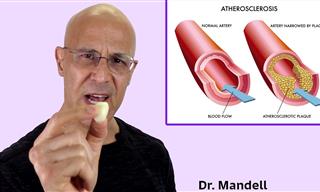
Here is something many people do not realize. A heart attack in a younger person is not always the same event, medically speaking, as one in an older person. In older adults, the usual cause is well understood: cholesterol plaque builds up in an artery over many years, then ruptures and forms a clot that blocks blood flow. This is the classic heart attack, and it remains the most common type even in younger patients.

But younger hearts are more likely to suffer heart attacks from causes that have nothing to do with that slow buildup of plaque. This matters a great deal, because the cause determines the treatment. One important example is a condition called spontaneous coronary artery dissection, in which the wall of a coronary artery suddenly tears. This is a leading cause of heart attacks in younger women in particular, accounting for a large share of cases in women under fifty, including those linked to pregnancy. Another is coronary spasm, where the artery clamps down hard and cuts off blood flow without any clot at all. There is also a category doctors call a heart attack with non-obstructive arteries, where the patient clearly has the signs of a heart attack but the arteries, on first look, appear open.
Recognizing these different causes is essential, because the standard heart attack treatment is not always the right one. A heart attack caused by a clot in a blocked artery is often treated by opening that artery and placing a small mesh tube called a stent. But for an artery that has torn on its own, placing a stent can sometimes do more harm than good, and many of these cases are best managed with medication and careful monitoring instead. A heart attack caused by spasm is treated with an entirely different family of drugs, ones that relax the artery walls. This is why younger patients often need a more thorough investigation, sometimes including advanced imaging inside the artery or detailed scans of the heart muscle, to be sure the real cause is found and the right treatment chosen. A young patient whose true cause is missed may be sent home without the care they actually need.
There is a hopeful side to all of this. Younger hearts often have more reserve and resilience, and many younger patients recover well, particularly when the cause is correctly identified and addressed. The key is taking the event seriously, both in the emergency room and in the months of recovery that follow.
The encouraging truth at the heart of this story is that most of these heart attacks are preventable. The same habits that protect an older heart protect a younger one, and the earlier they begin, the more powerful they become.
The foundation is simple and familiar. A diet built around vegetables, fruits, whole grains, and healthy fats, in the spirit of the Mediterranean way of eating, does more for the heart than almost anything else. Regular movement matters enormously, and it does not require a gym membership or punishing workouts. A daily walk, taken seriously and kept up, is one of the finest gifts a person can give their heart. Not smoking, going easy on alcohol, getting enough sleep, and finding real ways to manage stress all add up over the years.

Then there is the part that younger people too often skip: knowing their numbers. Blood pressure, cholesterol, and blood sugar can all drift into dangerous territory without producing a single symptom. A young adult can feel perfectly healthy while trouble quietly takes root. Doctors now recommend that cholesterol checks begin in early adulthood, and that anyone with a family history of early heart disease have an honest conversation with their physician about it. For those with extra risk, there are additional tests and screenings that can reveal hidden danger long before it becomes an emergency. The message to pass along to the younger people in your life is this: do not wait for symptoms, because by the time the heart speaks up, the conversation is already far along.
If you have grown children or grandchildren, this may be one of the more valuable things you can share with them. They are the generation living through this shift, often without realizing it, and a gentle nudge to get a checkup, take a daily walk, or simply not brush off a worrying symptom could one day matter more than any of us would like to imagine. Hearts, young and old alike, respond beautifully to care. The sooner that care begins, the longer and stronger they tend to beat.
Aggarwal R, Yeh RW, Joynt Maddox KE, Wadhera RK. "Cardiovascular Risk Factor Prevalence, Treatment, and Control in US Adults Aged 20 to 44 Years, 2009 to March 2020." JAMA. 2023;329(11):899-909. https://pubmed.ncbi.nlm.nih.gov/36871237/
Kamel I, et al. "Myocardial Infarction and Cardiovascular Risks Associated With Cannabis Use: A Multicenter Retrospective Study." JACC: Advances. 2025. https://www.acc.org/About-ACC/Press-Releases/2025/03/17/15/35/Cannabis-Users-Face-Substantially-Higher-Risk
Northwestern Medicine. "The Rise in Heart Attacks in People Under 40" (summarizing American College of Cardiology data on the roughly two percent annual rise). https://www.nm.org/healthbeat/healthy-tips/the-rise-in-heart-attacks-in-people-under-40
American Heart Association Scientific Statement. "Contemporary Diagnosis and Management of Patients With Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease (MINOCA)." Circulation. https://www.ahajournals.org/doi/10.1161/CIR.0000000000000670
Canadian Cardiovascular Society / Canadian Women's Heart Health Alliance. "Clinical Practice Update on Myocardial Infarction With No Obstructive Coronary Artery Disease (MINOCA)." Canadian Journal of Cardiology. 2024. https://onlinecjc.ca/article/S0828-282X(24)00207-1/fulltext
"Acute Myocardial Infarction: Etiologies and Mimickers in Young Patients." Journal of the American Heart Association. https://www.ahajournals.org/doi/10.1161/JAHA.123.029971