Polycythemia vera (PV) is a rare blood disorder that affects approximately 2-3 people per 100,000 individuals worldwide. Despite its rarity, understanding this condition is crucial for those diagnosed with it and their families. This comprehensive guide will walk you through what polycythemia vera is, its causes, symptoms, treatment options, and what the future holds for patients living with this condition.
What is Polycythemia Vera?
Polycythemia vera is a type of blood cancer classified as a myeloproliferative neoplasm (MPN). The name literally means "many blood cells that are true" – and that's exactly what happens in this condition. Your bone marrow, which is responsible for producing blood cells, goes into overdrive and creates too many red blood cells, and often too many white blood cells and platelets as well.
Think of your bone marrow as a factory that's supposed to produce a balanced number of different blood cell types. In polycythemia vera, the factory's controls malfunction, and it starts overproducing, particularly red blood cells. This overproduction makes your blood thicker than normal, similar to how adding too much flour to cake batter makes it harder to mix and pour.
This thickened blood can cause serious complications because it doesn't flow through your blood vessels as easily as normal blood. It's like trying to push honey through a straw instead of water – everything slows down, and blockages can occur.
The vast majority of polycythemia vera cases – about 95% – are caused by a specific genetic mutation called JAK2 V617F. This mutation occurs in a gene that normally helps control blood cell production. When this gene mutates, it sends constant "go" signals to blood-producing cells, telling them to keep making more cells even when the body doesn't need them.
It's important to understand that this mutation is acquired, not inherited. This means you don't get it from your parents, and you won't pass it on to your children. The mutation typically develops later in life, which is why polycythemia vera most commonly affects people over 60, though it can occur in younger adults.
Scientists don't yet fully understand what triggers this mutation to occur. It appears to be a random cellular event rather than something caused by lifestyle factors, environmental exposures, or other controllable circumstances. This can be both frustrating and reassuring for patients – frustrating because there's nothing they could have done to prevent it, but reassuring because it's not something they caused.
Polycythemia vera symptoms develop gradually and can be subtle at first, which is why the condition is sometimes discovered during routine blood tests before symptoms become noticeable. The symptoms are primarily related to having too many blood cells and blood that's thicker than normal.
Fatigue and weakness are among the most common early symptoms. Paradoxically, even though you have more red blood cells (which carry oxygen), you may feel tired because the thickened blood doesn't circulate efficiently.
Headaches and dizziness occur because the brain isn't receiving optimal blood flow. Some patients describe feeling like they're in a fog or having difficulty concentrating.
Itching, especially after warm baths or showers, affects about 40% of patients. This happens because the excess blood cells release chemicals that irritate nerve endings in the skin.

Vision problems can include blurred vision, blind spots, or seeing flashing lights. These occur when small blood vessels in the eyes become blocked or damaged.
High blood pressure develops because the heart has to work harder to pump the thickened blood through the circulatory system.
Enlarged spleen (splenomegaly) happens in about 70% of patients. You might feel fullness or pain in the upper left side of your abdomen, or feel full quickly when eating.
Blood clots are one of the most serious complications, occurring in about 20-30% of patients at diagnosis. These can happen anywhere in the body but commonly affect legs (deep vein thrombosis), lungs (pulmonary embolism), or brain (stroke).
Some patients also experience unusual symptoms like burning pain in hands and feet, night sweats, unexplained weight loss, or frequent infections.
Diagnosis typically begins with blood tests that show elevated levels of red blood cells, measured by hematocrit (the percentage of blood volume made up of red blood cells) and hemoglobin levels. However, high red blood cell counts can have other causes, so additional testing is needed.
The key diagnostic test is checking for the JAK2 mutation through genetic testing. Finding this mutation, combined with elevated blood counts and other clinical criteria, confirms the diagnosis in most cases.
Additional tests might include bone marrow biopsy, which shows increased cell production, and measurements of erythropoietin (EPO), a hormone that stimulates red blood cell production. In polycythemia vera, EPO levels are typically low because the body is trying to slow down red blood cell production.
Treatment for polycythemia vera aims to reduce the risk of blood clots and manage symptoms while maintaining quality of life. The approach is typically tailored to individual risk factors, age, and overall health.
How it works: Regular removal of blood, similar to blood donation, reduces the number of red blood cells and decreases blood thickness. During the procedure, typically 450-500ml of blood (about one pint) is removed through a needle in your arm, just like donating blood. This immediately reduces your hematocrit level (the percentage of red blood cells in your blood). Your body responds by using iron stores to make new red blood cells, but since you have polycythemia vera, it takes time for the excess cells to build up again. The goal is to keep your hematocrit below 45% for men and 42% for women, which significantly reduces the risk of blood clots while maintaining enough red blood cells for normal oxygen delivery.

Advantages:
Disadvantages:
How it works: Reduces the risk of blood clots by making platelets less sticky. Aspirin permanently blocks an enzyme called cyclooxygenase-1 (COX-1) in platelets, which prevents them from producing thromboxane A2, a chemical that normally makes platelets clump together. Since polycythemia vera patients often have elevated platelet counts and overactive platelets, this "anti-sticky" effect is particularly beneficial. The dose used (typically 81-100mg daily, much lower than pain-relief doses) is enough to block platelet function without completely preventing normal blood clotting. Each platelet remains affected for its entire 7-10 day lifespan, which is why the effect persists even with once-daily dosing.

Advantages:
Disadvantages:
How it works: A chemotherapy medication that slows down bone marrow production of blood cells. Hydroxyurea interferes with DNA synthesis during cell division by inhibiting an enzyme called ribonucleotide reductase, which is essential for making the building blocks of DNA. When cells in the bone marrow try to divide and create new blood cells, they can't complete the process properly, so fewer cells are produced. This affects all types of blood cells, but the impact is most noticeable on the rapidly dividing cells that produce red blood cells, white blood cells, and platelets. The medication is taken orally, usually once daily, and the dose is adjusted based on blood counts to find the right balance between controlling the disease and maintaining adequate blood cell levels.

Advantages:
Disadvantages:
How it works: A naturally occurring protein that helps regulate immune system and blood cell production. Interferon alpha is a cytokine (cell signaling protein) that your body normally produces in small amounts to fight infections and regulate cell growth. When given as medication, it works through multiple mechanisms: it directly inhibits the growth of abnormal blood cell-producing cells in the bone marrow, enhances the immune system's ability to recognize and eliminate abnormal cells, and may help restore more normal cell production patterns. Interferon also appears to specifically target cells carrying the JAK2 mutation, potentially reducing the burden of mutated cells over time. The medication is given by injection under the skin, with newer pegylated forms requiring less frequent dosing (weekly or every two weeks) because they remain active in the body longer.

Advantages:
Disadvantages:
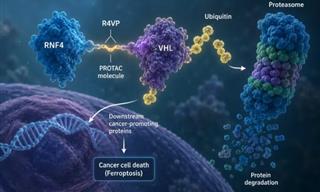
How it works: Specifically targets the JAK2 pathway that's overactive in polycythemia vera. The JAK2 protein normally acts like a molecular switch that turns on blood cell production when the body needs it. In polycythemia vera, the mutated JAK2 protein is stuck in the "on" position, constantly signaling for more blood cell production. Ruxolitinib is designed to fit precisely into the JAK2 protein and block its activity, essentially turning down the overactive switch. This helps restore more normal blood cell production levels. The drug also blocks related proteins (JAK1), which helps reduce inflammation and may shrink an enlarged spleen. Unlike chemotherapy drugs that broadly slow down cell division, JAK2 inhibitors are more targeted, specifically addressing the root molecular problem in polycythemia vera. The medication is taken orally twice daily, and the dose can be adjusted based on response and side effects.

Advantages:
Disadvantages:
The prognosis for polycythemia vera has improved significantly over the past few decades with better understanding and treatment of the condition. With proper management, many patients live normal or near-normal lifespans.
Life expectancy varies depending on age at diagnosis, overall health, and how well the condition responds to treatment. Studies suggest that patients diagnosed in their 60s might have a life expectancy 10-20 years shorter than average, but many patients live well into their 80s and beyond. Younger patients at diagnosis generally have better long-term outcomes.
Quality of life can be maintained with proper treatment. While some patients experience ongoing fatigue or other symptoms, many are able to continue working, traveling, and enjoying their usual activities.
Potential complications to be aware of include progression to more serious blood cancers (acute leukemia in 2-5% of patients, or myelofibrosis in 10-15% of patients), but these transformations typically occur many years after diagnosis and may be related to treatment choices.
Regular monitoring is essential and typically includes blood tests every 3-6 months, annual physical exams, and periodic imaging studies to check spleen size. Most patients develop a routine with their healthcare team that becomes manageable over time.
Research into polycythemia vera is active and promising. Scientists are investigating new JAK inhibitors that might be more effective or have fewer side effects. Gene therapy approaches are being explored, though these remain experimental.
Researchers are also studying combination therapies that might provide better disease control, and investigating ways to predict which patients might benefit most from specific treatments.
Understanding of the molecular biology of polycythemia vera continues to evolve, which may lead to more targeted and personalized treatment approaches in the future.
While receiving a diagnosis of polycythemia vera can be overwhelming, it's important to remember that this is a manageable condition for most patients. With proper treatment and monitoring, many people with PV continue to live full, active lives.
The key is working closely with a hematologist who specializes in blood disorders to develop a treatment plan that's right for your specific situation. Treatment is highly individualized, and what works best can vary from person to person.
Stay informed about your condition, but also remember that medical research is constantly evolving. What we know about polycythemia vera today is far more than we knew even a decade ago, and the outlook for patients continues to improve.
If you've been diagnosed with polycythemia vera, consider connecting with patient support groups or organizations like the MPN Research Foundation, which can provide additional resources and connect you with others who understand what you're experiencing.